

Introduction
Severe hemophilia A (SHA) is characterized by spontaneous (non-trauma related) bleeding episodes into the joint space and muscle tissue, leading to progressive joint deterioration and chronic pain. Chronic joint damage is most often associated with severe hemophilia, however more recent research has illustrated that people with moderate hemophilia A (MHA) also experience hemophilic arthropathy and functional impairment. The need to measure joint health in children as well as adults, is underscored by findings from the Joint Outcome Continuation Study, which found that FVIII prophylaxis was insufficient to protect joints from damage, from childhood through adolescence in severe HA (Warren et al., 2020).
The objective of this analysis is to gain a more patient-centric understanding of the clinical, economic and humanistic burden associated with 'Problem Joints', a measure of joint morbidity developed in consultation with an expert panel to overcome limitations with existing measures, in people with MHA and SHA.
Methods
A descriptive cohort analysis was conducted, utilizing retrospective, cross-sectional real-world data from the 'Cost of Haemophilia in Europe: a Socioeconomic Survey' (CHESS Paeds and CHESS II), studies of adult and pediatric persons with hemophilia. The analysis population is comprised of children (17 and below) with MHA or SHA in CHESS Paeds, and adults aged 20 and over with MHA or SHA in CHESS II. To account for the possibility that persons aged 18 or 19 in CHESS II may have participated in CHESS Paeds, these individuals were excluded from the analysis.
Physician-reported clinical outcome data and patient/caregiver-reported quality of life were analyzed. A problem joint (PJ) is defined as having chronic joint pain and/or limited range of movement due to compromised joint integrity (i.e. chronic synovitis and/or hemophilic arthropathy). Analyses were stratified by number of PJs: none, 1 PJ, and 2+ PJs. We report retrospective data of the 12 months prior to study enrollment, on annualized bleeding rate (ABR), prevalence of target joints (TJ), as defined by the International Society on Thrombosis and Haemostasis, and EQ-5D-/5L/Y/Proxy score. Results are presented as mean (standard deviation) or N (%).
Results
Among 785 participants (N = 464 SHA; N = 321 MHA) in CHESS Paeds, mean age and BMI were 10.33 (4.63) and 22.50 (17.07), respectively. Of 493 participants (aged 20 and above) in CHESS II (N = 298 SHA; N = 195 MHA), the mean age and BMI were 38.61 (14.06) and 24.55 (2.92), respectively. Current inhibitor to FVIII replacement was more prevalent in children than in adults (10% vs. 5%).
In CHESS II, approximately 40% of people with MHA and 49% with SHA had one or more PJs, respectively [1 PJ (23% vs. 28%); 2+ PJs (16% vs. 21%)]. In CHESS Paeds, approximately 14% of children with MHA and 18% with SHA had at least one PJ, respectively [1 PJ (9% vs. 14%); 2+ PJs (5% vs. 3%)]. TJs were less prevalent with MHA in comparison to SHA, in both adults (24% vs. 45%) and children (13% vs. 22%).
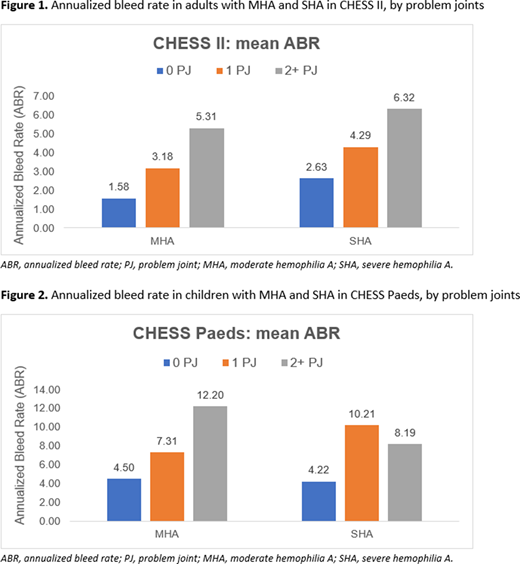
Clinical burden was higher among both children and adults with PJs compared to those with no PJs. ABR correlates with the number of PJs, in those with MHA and SHA in CHESS II (Figure 1). Similarly, PJs were associated with higher ABR across MHA and SHA in CHESS Paeds (Figure 2).
Hemophilia-related hospitalizations were higher in both adult and pediatric participants with PJs. In CHESS II, MHA with no PJs had fewer [0.73 (1.23)] hospitalizations compared to having those with 1 PJ [1.38 (1.11)] or 2+ PJs [1.28 (1.25)]. Similarly, children with MHA with 2+ PJs had 1.60 (1.92) hemophilia-related hospitalizations, compared to 1.38 (1.92) with 1 PJ and 0.71 (1.14) with no PJs.
PJs were associated with impaired quality of life. In CHESS II, MHA and SHA EQ-5D-5L values in persons with no PJs were 0.81 (0.19) and 0.79 (0.18), respectively, compared to 0.65 (0.16) and 0.62 (0.23) with 1 PJ, and 0.65 (0.14) and 0.51 (0.33) in with 2+ PJs. A similar trend was observed in EQ-5D-Y and EQ-5D-proxy scores in CHESS Paeds.
Conclusions
Data from CHESS Paeds and CHESS II demonstrate an association between chronic joint damage, as measured by the 'problem joint' definition, and worsening clinical and quality of life outcomes, across both MHA and SHA. Further analyses will seek to expand upon the initial results presented here, to investigate the wider elements of burden associated with compromised long-term joint health.
McLaughlin:BioMarin: Consultancy; Novo Nordisk: Consultancy, Speakers Bureau; Sobi: Consultancy, Speakers Bureau; Roche/Chugai: Speakers Bureau; Takeda: Speakers Bureau. Hermans:Novo Nordisk: Consultancy, Speakers Bureau; Roche: Consultancy, Speakers Bureau; Sobi: Consultancy, Research Funding, Speakers Bureau; Biogen: Consultancy, Speakers Bureau; CAF-DCF: Consultancy, Speakers Bureau; CSL Behring: Consultancy, Speakers Bureau; Shire, a Takeda company: Consultancy, Research Funding, Speakers Bureau; Pfizer: Consultancy, Research Funding, Speakers Bureau; Bayer: Consultancy, Research Funding, Speakers Bureau; WFH: Other; EAHAD: Other; Octapharma: Consultancy, Speakers Bureau; Kedrion: Speakers Bureau; LFB: Consultancy, Speakers Bureau. Asghar:HCD Economics: Current Employment. Burke:HCD Economics: Current Employment; University of Chester: Current Employment; F. Hoffmann-La Roche Ltd: Consultancy. Nissen:GSK: Research Funding; Novartis: Research Funding; Actelion: Consultancy; F. Hoffmann-La Roche Ltd: Current Employment. Aizenas:F. Hoffmann-La Roche Ltd: Current Employment, Current equity holder in publicly-traded company. Meier:F. Hoffmann-La Roche Ltd: Current Employment, Current equity holder in publicly-traded company. Dhillon:HCD Economics: Current Employment; F. Hoffmann-La Roche Ltd: Other: All authors received editorial support for this abstract, furnished by Scott Battle, funded by F. Hoffmann-La Roche Ltd, Basel, Switzerland. . O'Hara:F. Hoffmann-La Roche Ltd: Consultancy; HCD Economics: Current Employment, Current equity holder in private company.

